When the Blood Analyzer Cannot Report the CBC
When the Blood Analyzer Cannot Report the CBC
Cold agglutinin syndrome in lymphoma
By William C. Aird, MD
Case Presentation
A 64-year-old man with a history of:
- diabetes mellitus
- end-stage renal disease
- living donor renal transplant (2008)
presented with two weeks of nausea, vomiting, abdominal pain, and weight loss.
Imaging revealed extensive retroperitoneal lymphadenopathy causing gastric outlet obstruction, highly concerning for lymphoma.
Laboratory testing demonstrated:
- Hemoglobin: 9.0 g/dL
- LDH: markedly elevated
- Uric acid: 15.1 mg/dL
- Ferritin: 2760 ng/mL
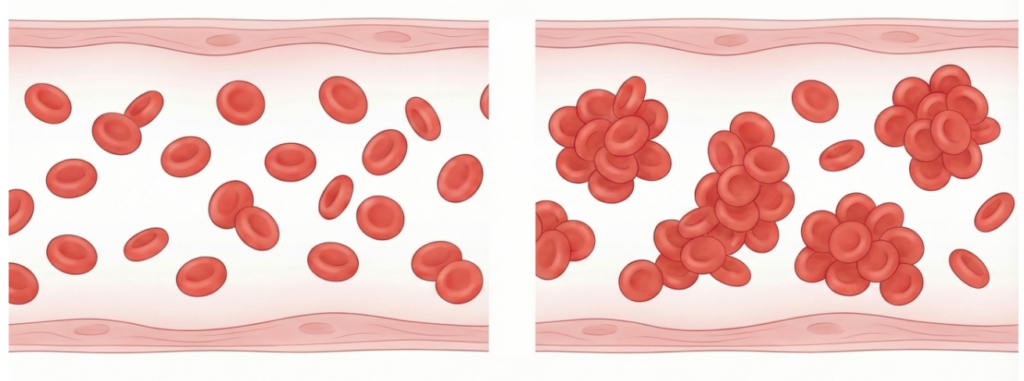
Peripheral blood smear also showed red cell agglutination, raising suspicion for cold agglutinin hemolysis associated with lymphoma.
Biopsy confirmed:
Monomorphic post-transplant lymphoproliferative disorder (PTLD), diffuse large B-cell lymphoma.

A Diagnostic Clue
During hospitalization, the laboratory reported:
“Unable to report RBC indices.”
The automated analyzer could not calculate:
- MCV
- MCH
- MCHC
- Hematocrit

When automated analyzers cannot report RBC indices, clinicians should consider whether red cells are clumping rather than circulating as individual cells.
Reviewing the peripheral smear and repeating the CBC on a warmed sample can help confirm this possibility.
