When disease burden justifies intervention
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
In cold agglutinin disease, knowing when not to treat is as important as knowing how to treat.
Many patients live for years with stable laboratory abnormalities and tolerable symptoms; some have compensated hemolysis or mild anemia without symptoms.1
Treating too early exposes patients to unnecessary risk. Treating too late prolongs avoidable morbidity.
There is no hemoglobin threshold, antibody titer, or laboratory value that dictates treatment. CAD treatment decisions are judgment-based, driven by clinical impact and disease trajectory. They reflect the dual biology of CAD: complement-mediated hemolysis and non–complement-mediated agglutination, which contribute differently to anemia, symptoms, and treatment priorities.2
In practice, access to certain therapies may still require laboratory thresholds for authorization, but these administrative criteria should not substitute for clinical judgment.
What treatment is trying to accomplish
Treatment in CAD is aimed at reducing clinically meaningful harm, not normalizing numbers in isolation.
Treatment is intended to:
- reduce clinically significant hemolysis
- improve symptoms and quality of life
- prevent recurrent exacerbations
- stabilize or reverse disease trajectory
Clinical trial response criteria emphasize improvements in hemoglobin, symptoms, and transfusion need rather than laboratory normalization alone.3
Different therapies pursue different goals. Complement-directed therapy primarily controls hemolysis, clone-directed therapy aims to suppress pathogenic IgM production, and supportive strategies mitigate consequences without altering the underlying mechanism. Choosing whether to treat is therefore partly a decision about what problem you are trying to solve.
When observation is appropriate
Many patients with CAD do not require immediate disease-directed therapy.4
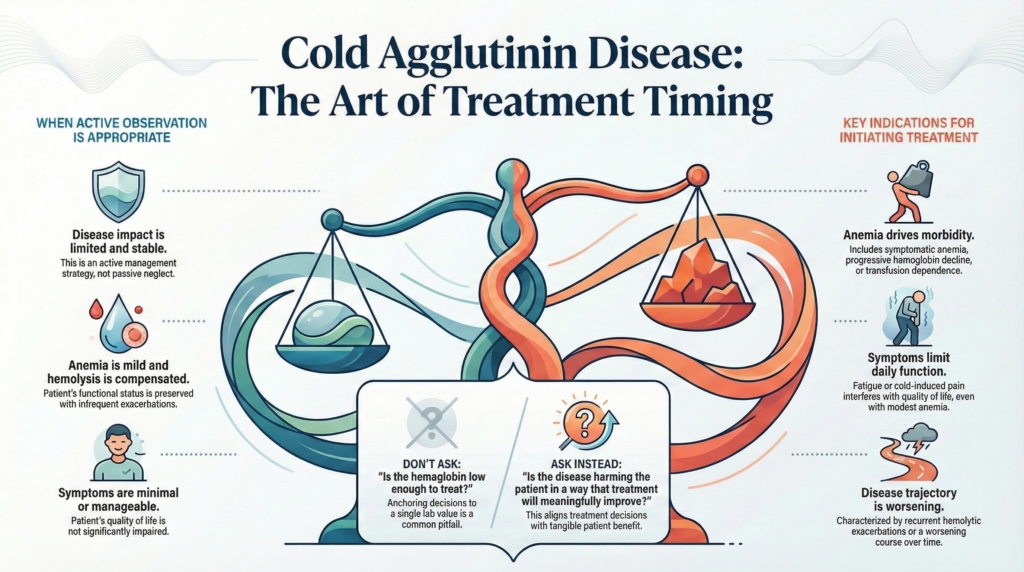
Observation is reasonable when disease impact is limited and stable.
Observation is appropriate when:
- anemia is mild and stable
- symptoms are minimal or manageable
- hemoglobin remains stable due to adequate erythropoietic compensation
- exacerbations are infrequent
- functional status is preserved
Management decisions are based primarily on anemia severity and symptom burden, and patients with mild or compensated anemia may not require treatment.5
Observation is not passive.
Active observation means structured follow-up with explicit thresholds — changes in symptoms, hemoglobin trajectory, or exacerbation frequency — that prompt reconsideration. These thresholds are shared with the patient in advance.
Indications for treatment
Treatment should be considered when CAD produces clinically meaningful harm.
Clinically meaningful harm may arise through anemia, disabling circulatory symptoms, or unfavorable disease behavior over time.
Anemia-related indications
When anemia itself drives morbidity or instability, treatment is justified, including:
- symptomatic anemia
- progressive decline in hemoglobin
- transfusion dependence
Published CAD cohorts report baseline hemoglobin values commonly around 9 g/dL, and transfusion exposure during the disease course is frequent.6
Symptom-driven indications
Symptoms matter even when laboratory abnormalities appear modest.
Typical manifestations of clinically significant anemia include fatigue, dyspnea, palpitations, and pallor.7
Because hemoglobin level alone may not capture clinical burden, the patient’s own assessment of functional impact is a critical input into treatment decisions.
Disabling cold-induced circulatory symptoms alone may justify treatment even when anemia is modest.
Disease behavior
Trajectory often matters more than snapshot severity, including:
- recurrent hemolytic exacerbations
- worsening disease course over time
- hemolysis that persists despite supportive measures
Febrile infections, trauma, or surgery can precipitate acute hemolytic exacerbations.8
Anemia severity is not the whole story
Hemoglobin level alone is an unreliable trigger for therapy in CAD.
Some patients tolerate low hemoglobin surprisingly well because of physiologic adaptation to chronic anemia.9
Treatment decisions should therefore integrate:
- hemoglobin trend rather than a single value
- trends in hemolysis markers (LDH, bilirubin, reticulocytes, haptoglobin)
- symptom burden
- functional impact
- disease stability over time
Clinical judgment in practice
A patient with hemoglobin 9.5 g/dL, stable over six months, compensated hemolysis, and manageable symptoms may be best managed with observation and follow-up.
The same hemoglobin in a patient with worsening fatigue, declining trend, or recurrent exacerbations may justify treatment.
The number is identical.
The decision is not.
A practical framing question
Instead of anchoring decisions to thresholds, reframe the question.
Rather than asking:
Is the hemoglobin low enough to treat?
Ask:
Is this disease currently harming the patient in a way that treatment is likely to meaningfully improve?
This keeps treatment aligned with benefit rather than numbers.
Cold avoidance alone is not a treatment test
Cold avoidance is important, but it is not a diagnostic or therapeutic litmus test.
In pathogenic CAD, hemolysis may persist despite preventive measures, and symptoms may occur year-round.10
Marked lifestyle restriction from cold avoidance may indicate clinically meaningful ongoing disease burden, even when anemia is modest.
Common reasons treatment is delayed inappropriately
Treatment is often postponed because disease impact is underestimated.
Common cognitive traps include:
- labeling anemia as “mild” despite high symptom burden
- over-reliance on modest hemolysis markers
- attributing symptoms only to cold exposure while underrecognizing the underlying IgM/complement-mediated process
- mistaking uncertainty for benignity
CAD does not always signal urgency through dramatic laboratory abnormalities.11
Common reasons treatment is started too early
Conversely, treatment may be initiated prematurely when biological context is misunderstood.
This most often occurs when:
- an isolated cold agglutinin is mistaken for CAD
- transient post-infectious hemolysis is assumed to be chronic disease
- asymptomatic laboratory abnormalities drive intervention
- fear of future worsening overrides current disease behavior
Not every patient with CAD requires therapy.12
Tempo matters
Most treatment decisions in CAD are not emergent.
However, rapid hemoglobin decline, severe symptomatic anemia, or acute hemolytic exacerbations may justify accelerated decision-making. Even then, urgency should guide tempo, not replace judgment.
Urgency may favor therapies with rapid onset. In selected cases, when the clinical picture is compelling, treatment may begin while diagnostic evaluation is being completed, with supportive care bridging the interval.
Teaching uncertainty without paralysis
Good practice involves:
- revisiting assumptions as disease evolves
- tolerating ambiguity without forcing premature decisions
- matching treatment intensity to disease behavior rather than labels
- communicating uncertainty honestly to patients
This is disciplined restraint, not indecision.
Deciding when to treat often requires acting without perfect information.
Explicit principle
Do not treat laboratory abnormalities in isolation.
Treat patients whose disease meaningfully interferes with health, function, or stability.
Mastery of when to treat in CAD is less about memorizing criteria and more about recognizing impact, trajectory, and burden over time.
Reflect and Apply
Think of a patient with CAD whose hemoglobin is abnormal but stable.
Before deciding whether to treat, ask:
Is the disease harming the patient now?
Through symptoms, functional limitation, transfusion need, recurrent exacerbations, or progressive hemolysis?
Is the current approach still acceptable?
To the patient, not just to the laboratory record?
Would treatment meaningfully improve health, function, or stability?
In CAD, the question is not:
Is the hemoglobin low enough?
It is:
Is the disease burden high enough to justify intervention?
Practice guidance: when treatment is indicated
Based on international guideline and consensus statements
Based on BSH guidance for primary AIHA, international consensus recommendations, and expert CAD reviews, observation is appropriate for patients with mild or minimally symptomatic CAD, particularly when hemolysis is compensated and disease burden is limited.
Treatment is generally considered when CAD produces clinically impactful disease, including symptomatic anemia, transfusion requirement, non-compensated or worsening hemolysis, marked fatigue attributable to CAD, or disabling cold-induced circulatory symptoms.
These sources support the central principle that treatment decisions should be based on clinical impact, symptom burden, and trajectory, rather than a single laboratory value.
Test your thinking
A short, judgment-focused quiz on timing of treatment in cold agglutinin disease.