Why environment, not immunity alone, shapes who suffers most
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Cold agglutinin disease is often framed as an immunologic problem with a thermal trigger.
That framing is correct, but incomplete.
Cold is not experienced equally.
While cold itself is not formally classified as a social determinant of health, the ability to avoid or mitigate cold is deeply shaped by the same structural forces—housing, work, transportation, and economic resources—that define social determinants more broadly.
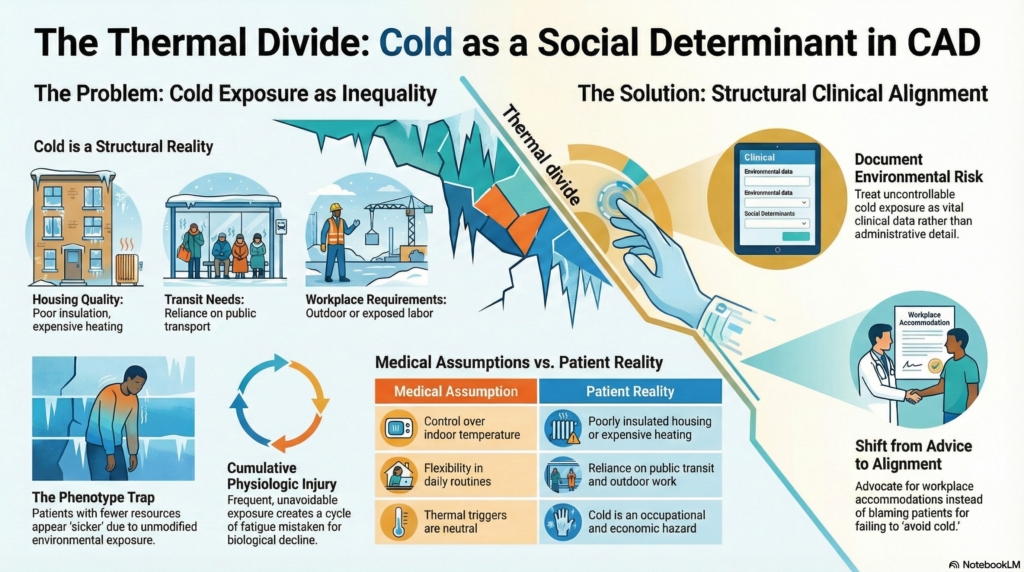
For patients with CAD, cold functions less like a neutral weather condition and more like a social determinant of health—not because cold itself is social, but because exposure to cold is unevenly structured by housing, work, geography, and resources.
Cold is not just temperature
In clinical discussions, cold is treated as a number: degrees Celsius, room temperature, outdoor climate. In lived experience, cold is contextual.
Cold means:
- poorly insulated housing
- unreliable heating
- long commutes or outdoor work
- drafty workplaces
- public transportation platforms
- air-conditioned offices, clinics, and stores
- limited ability to control one’s environment
For patients with CAD, these are not inconveniences. They are repeated physiologic insults.
Cold exposure accumulates. And accumulation is shaped by circumstance.
When cold becomes a social determinant
Not all cold is a social determinant.
Cold exposure in CAD is heterogeneous: it may be structural, occupational, geographic, recreational, or iatrogenic, but it becomes a social determinant when patients lack meaningful control over it.
Winter in Minnesota is weather.
But the inability to stay warm indoors is structural.
The requirement to work in cold environments is occupational.
The lack of control over temperature is economic.
Cold becomes a social determinant when patients cannot modify exposure without sacrificing housing, income, safety, or dignity.
That distinction matters, because it determines whether the solution is medical advice—or structural accommodation.
Housing and thermal control
The ability to stay warm is not evenly distributed.
Some patients can adjust thermostats freely, wear layers without consequence, work remotely, or relocate seasonally. Others cannot. They live in older buildings, shared housing, or climates where heating is expensive, inconsistent, or rationed.
In CAD, the gap between “avoid cold” as advice and “avoid cold” as reality can be wide.
Medical recommendations quietly assume:
- control over indoor temperature
- access to warm clothing
- flexibility in daily routines
When those assumptions fail, it is not the patient who has failed.
It is the care model.
Work, exposure, and invisible risk
Occupational exposure matters.
Patients who work outdoors, in warehouses, in food service, in healthcare, or in tightly climate-controlled environments may face daily cold exposure that cannot be negotiated away. Asking such patients to “avoid cold” can amount to asking them to risk employment.
Cold becomes a workplace hazard that is rarely documented, accommodated, or acknowledged.
Medicine is comfortable naming chemical, infectious, and ergonomic risks at work. It is far less comfortable naming thermal risk, even when disease physiology is explicitly temperature-dependent.
CAD exposes that blind spot.
Some cold exposures occur in environments patients cannot refuse, including clinical settings themselves.
Geography and the accident of place
Where a patient lives can shape disease expression as much as disease biology.
Two patients with identical antibodies and hemoglobin levels may live profoundly different lives depending on latitude, climate, and infrastructure. Rural cold is not urban cold. Coastal cold is not alpine cold. Winter is not the same everywhere.
Wind exposure, transit patterns, building insulation, and time spent outdoors vary dramatically by place.
Yet clinical guidance rarely adjusts for geography beyond vague seasonal advice.
In CAD, cold behaves much like altitude does in pulmonary disease: a contextual modifier that determines who becomes symptomatic, when, and how severely. The difference is not biology. It is exposure.
Cold exposure as cumulative harm
Cold does not harm CAD patients once. It harms them repeatedly.
Each exposure:
- worsens circulation
- increases fatigue
- restricts activity
- reinforces avoidance
Over time, this creates cumulative limitation that can look like gradual decline. But it is not inevitable progression. It reflects repeated environmental stress.
Without recognizing this, clinicians may escalate therapy when the true driver is exposure.
When clinicians attribute worsening solely to disease biology, they may miss an upstream driver that cannot be fixed with medication alone.
Inequity disguised as biology
Because CAD is biologically mediated, disparities in experience can masquerade as differences in disease severity.
Patients with fewer resources may appear “sicker,” “more symptomatic,” or “less resilient,” when in fact they are simply more exposed. The disease declares itself where protection fails.
This creates what might be called a phenotype trap: environmental disadvantage masquerading as biological severity.
The result is a quiet injustice:
- those with less control over environment bear more burden
- those with more control appear to have milder disease
Without naming cold as a social determinant, medicine risks mistaking inequity for phenotype.
What recognizing cold changes
Recognizing cold as a social determinant does not require clinicians to solve housing or climate inequity. It requires something more modest—and more powerful: recognition.
It changes how clinicians:
- interpret symptom severity
- evaluate response to treatment
- assess “failure” of conservative measures
- counsel patients realistically
- advocate for accommodations
It reframes “nonadherence” as constraint, and “progression” as exposure.
From advice to alignment
Telling patients with CAD to “avoid cold” is easy. Helping them navigate a world that is not built for thermal vulnerability is harder.
Ethical care lies in the space between.
That space includes:
- asking where and how patients live
- asking what cold exposure they cannot avoid
- documenting environmental risk
- supporting workplace and procedural accommodations
- adjusting expectations, not just medications
In practice, this means asking not only “Do your symptoms worsen in cold?” but also “Where are you exposed to cold that you cannot control?” Documenting these constraints in the medical record is not administrative detail. It is clinical data. Such documentation can support workplace accommodations, procedural modifications, and environmental adjustments that medication alone cannot achieve.
Cold is not neutral.
Neither is the world patients move through.
What CAD reveals
Cold agglutinin disease reminds us that environment does not merely modify disease. It distributes it.
Cold behaves like a social determinant precisely because it is unevenly encountered, unevenly controlled, and unevenly mitigated. When medicine ignores that fact, it risks turning environmental vulnerability into invisible blame.
CAD reveals a broader lesson:
Some diseases are not just carried in blood.
They are carried through buildings, jobs, cities, and winters.
Recognizing that is not sociology for its own sake.
It is clinical accuracy.
Clinical implications
- cold exposure is structurally distributed — housing, work, and geography shape physiologic burden
- unequal exposure can masquerade as phenotype — resource differences may appear as disease severity
- “avoid cold” assumes environmental control — recommendations must align with lived constraints
- environmental documentation is clinical data — recording exposure supports accommodation and planning
- recognition precedes intervention — naming cold as a determinant changes interpretation before it changes treatment
Clinical Documentation Note
For patients with CAD, document cold exposure as clinical context, not lifestyle detail. Relevant exposures may include housing temperature, heating insecurity, outdoor work, refrigerated or air-conditioned workplaces, public transportation, procedural environments, and inability to modify temperature safely or affordably.
This documentation can support accommodations and prevent mislabeling exposure-driven symptoms as disease progression or nonadherence.
Reflect and Apply
A patient with CAD reports worsening winter fatigue and missed workdays.
Before escalating therapy, ask:
Where is this patient exposed to cold that they cannot control?
Is the exposure coming from housing, work, transportation, clinical settings, or financial constraints?
What would change if you documented this not as “poor cold avoidance,” but as environmental disease burden?
That is still compact, but it better captures the essay’s argument.
Additional reading
- Healthy People 2030: Social Determinants of Health
- Vrtikapa K et al. Social Determinants of Health: The Impact of This Overlooked Vital Sign. J Brown Hosp Med. 2025.
- Joly F et al. The Burden of Cold Agglutinin Disease on Patients’ Daily Life: Web-Based Cross-sectional Survey of 50 American Patients. JMIR Form Res. 2022.
- Winter Is No ‘Wonderland’ for People With CAD
- Hansen et al. Mortality in cold agglutinin disease shows seasonal pattern. Transfusion. 2022.
- Seasonal patterns of thromboembolic events in CAD
- Healthy People 2030 SDOH documentation framework
- Practice‑oriented SDOH/clinical documentation guidance