For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
A guide for patients with essential thrombocythemia (ET)
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
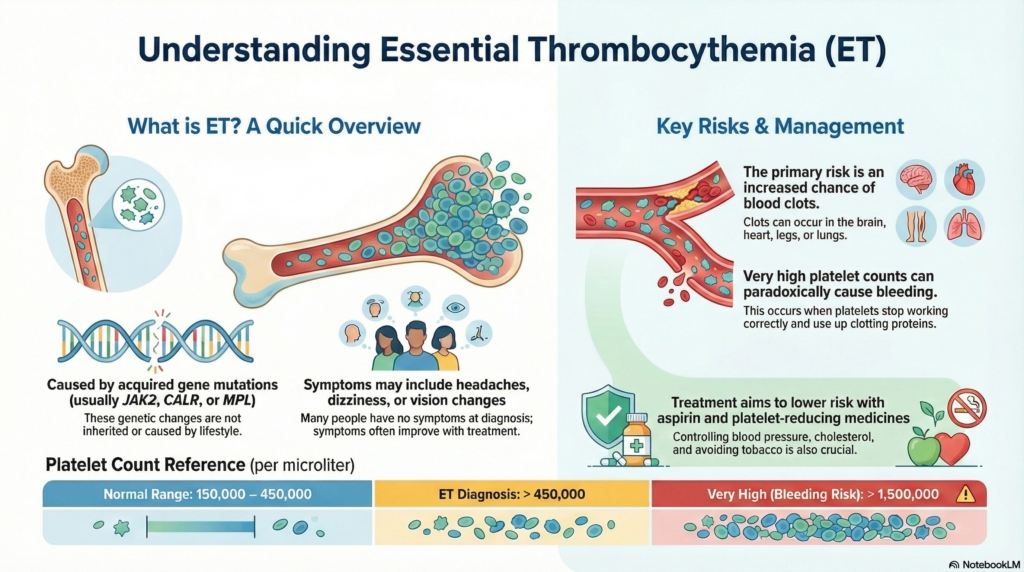
Essential thrombocythemia (ET) is a chronic blood condition in which the bone marrow makes too many platelets, which can increase the risk of blood clots and, when counts are very high, bleeding.
With the right treatment and regular follow-up, most people with ET live long, active lives while keeping complications to a minimum.
This information is for general education and does not replace medical care. It applies to people who are medically stable. If you are experiencing new or worsening symptoms, contact your doctor or seek emergency care.
First things first
Essential thrombocythemia is a myeloproliferative neoplasm, a chronic blood cancer in which the bone marrow produces too many platelets. Platelets normally help the blood clot and repair injured blood vessels. In ET, the platelet count can climb so high that it increases the risk of blood clots, and at very high levels, platelets may not work properly and can actually increase the risk of bleeding.
Most people with ET feel well at the time of diagnosis. ET is typically a slow-moving condition, and with appropriate treatment and monitoring, many people remain stable for decades.
What is essential thrombocythemia?
In ET, the bone marrow makes more platelets than the body needs. This is usually driven by changes in genes that regulate blood cell growth. The most common are JAK2, CALR, and MPL mutations.
These gene changes:
- are acquired during life (not something you were born with)
- are not caused by anything you did or did not do
- cause persistent elevation in platelet count
About 10% some people with ET have none of these three mutations; this is sometimes called “triple-negative” ET. In those cases, a bone marrow biopsy and other specialized tests become especially important to confirm the diagnosis and rule out related conditions.
ET is usually long-term but very treatable. Many people never develop serious complications.
Why it happens (causes)
ET is caused by changes in genes that control how blood-forming cells grow and divide. Mutations in JAK2, CALR, or MPL send strong “grow” signals even when the body does not need more platelets.
Key points:
- these mutations are acquired, not inherited in the usual sense
- ET is not caused by diet, exercise, stress, or lifestyle choices
- ET is not contagious and cannot be passed from person to person
Does it cause symptoms?
Many people with ET have no symptoms at first. Others notice patterns that are typical for ET, especially related to small blood vessels (microvascular symptoms). These can include:
- headaches or a feeling of pressure in the head
- lightheadedness or dizziness
- numbness, tingling, or burning in the hands or feet
- vision changes, such as flashing lights, blurry spots, or zigzag patterns
- reddened, warm, painful hands or feet (erythromelalgia) that often improve with aspirin
- fatigue or low energy
- fullness or discomfort in the left upper abdomen from an enlarged spleen
- easy bruising, nosebleeds, or bleeding from gums when platelets are extremely high
These symptoms often improve once platelet counts are brought into a safer range and, in many cases, when low-dose aspirin is started.
Is it dangerous?
The main concern in ET is an increased risk of blood clots. Clots can form in:
- arteries in the brain, causing stroke-like symptoms
- arteries of the heart, causing chest pain or heart attack–like symptoms
- veins in the legs (deep vein thrombosis)
- veins in the lungs (pulmonary embolism)
- veins in the abdomen or liver (less common but serious)
Doctors classify ET as low-risk or high-risk based on:
- age (higher risk if 60 or older)
- history of blood clots
- presence of the JAK2 mutation, which is associated with higher clot risk
Understanding the bleeding risk
When platelet counts become extremely high (often above about 1,500,000), platelets can stop working properly. They may use up certain clotting proteins faster than the body can replace them or cause a specific defect called acquired von Willebrand syndrome. In that setting, even though the platelet count is high, the blood may be more prone to bleeding, such as nosebleeds, easy bruising, bleeding gums, or gastrointestinal bleeding. This is less common than clotting but important to recognize, and it is one reason that very high platelet counts usually prompt more aggressive treatment and careful decisions about aspirin use.
Over many years, a small percentage of people with ET (on the order of a few people out of every hundred over a decade or more) can develop myelofibrosis, in which the bone marrow becomes scarred and less efficient, or, rarely, acute leukemia. These complications are uncommon, especially with modern therapies and regular follow-up, but they are part of why lifelong monitoring is essential.
How your doctor evaluates it
Evaluation usually includes:
- blood tests measuring platelet count, hemoglobin, hematocrit, and white blood cells
- genetic testing for JAK2, CALR, and MPL mutations
- review of your personal and family history of clots or bleeding
- physical examination, especially checking for an enlarged spleen
- iron studies, since iron deficiency can also raise platelet counts
- sometimes a bone marrow biopsy to confirm the diagnosis and distinguish ET from other myeloproliferative neoplasms or reactive causes
To give context:
counts above about 1,500,000 are considered very high and often require more urgent attention because of both clot and bleeding risks.
How is it treated
Treatment focuses on lowering clot risk, reducing symptoms, and keeping platelet counts in a safer range.
Low-dose aspirin
Aspirin helps reduce microvascular symptoms (such as headaches, erythromelalgia, and vision changes) and lowers clot risk in many people with ET.
- it is commonly recommended, especially for those with symptoms or cardiovascular risk factors
- in very low-risk patients (younger, no JAK2 mutation, no prior clots, no symptoms), the decision to use aspirin is individualized
- if significant bleeding occurs or platelet counts become extremely high, your doctor may temporarily stop aspirin while the bleeding risk is evaluated
Platelet-lowering medicines (cytoreductive therapy)
These medicines are used when clot risk is higher or when platelets are very high or causing symptoms. They include:
- hydroxyurea, an oral medicine often used as first-line treatment in many adults
- interferon, often favored in younger adults or during pregnancy planning
- anagrelide, used in selected cases, often when other medicines are not suitable
Doctors pay particular attention to:
- high-risk features (age 60 or older, prior clot, JAK2 mutation)
- very high platelet counts (often above 1,500,000)
- troublesome symptoms or bleeding
Controlling cardiovascular risk factors
Because clots in ET are influenced by general cardiovascular health, it is crucial to:
- control blood pressure, cholesterol, and diabetes
- avoid tobacco
- address other risk factors such as obesity and inactivity
Treatment choices and goals are tailored to you and may change over time as your situation evolves.
Daily life and self-care
Most people with ET can work, exercise, travel, and enjoy family and social life. Helpful steps include:
Staying active and mobile
Regular moderate exercise is encouraged and may help reduce clot risk. Normal activities are usually fine. During long car rides or flights, stand, stretch, and walk periodically to keep blood moving. If your platelet count is extremely high or you have bleeding concerns, your doctor may advise avoiding contact sports or activities with high injury risk.
Staying well hydrated
Drinking fluids regularly can help support healthy blood flow. This is especially important during hot weather, when you are ill, or when you are less active.
Managing cardiovascular risk
Work with your care team to control blood pressure, cholesterol, and diabetes, and avoid smoking completely.
Understanding iron and ET
Iron deficiency can also raise platelet counts. Your doctor will check iron levels as part of your evaluation. Treating iron deficiency may lower platelet counts in some people, but it does not cure ET, since ET is driven by the marrow condition itself. If you have signs of bleeding (such as black stools) or are on aspirin, your doctor may look for sources of blood loss.
Pregnancy and ET
ET can affect pregnancy, so planning is important:
- risks can include higher chances of miscarriage, clotting, and placental problems
- medicines such as hydroxyurea and anagrelide are generally avoided in pregnancy
- interferon is often preferred if platelet-lowering treatment is needed
- low-dose aspirin is commonly continued, and in some cases blood thinners are added during or after pregnancy
Successful pregnancies are common when ET is managed jointly by a hematologist and a high-risk obstetrician, with careful planning and close monitoring.
When should I contact my doctor?
Call your hematologist or clinic promptly if you have:
- new or worsening headaches, dizziness, or vision changes
- new chest discomfort, breathlessness, or palpitations
- new leg pain, redness, or swelling
- increasing discomfort or fullness under the left ribs
- unusual or heavy bleeding
- fevers, night sweats, or unexplained weight loss
- a clear change in your usual PV symptoms
Call 911 or go to an emergency department if you have:
- stroke-like symptoms (face drooping, arm weakness, trouble speaking)
- sudden chest pain, pressure, or difficulty breathing
- coughing up blood
- sudden severe leg swelling or pain
- sudden severe abdominal pain
- bleeding that will not stop with pressure
Tell emergency staff that you have polycythemia vera and which medicines you take.
What is the usual plan going forward?
ET is a lifelong condition. Over time, your care plan usually includes:
- regular blood tests to track platelet count, hemoglobin, and white blood cells
- adjustments in aspirin and platelet-lowering medicines based on your risk and counts
- ongoing attention to cardiovascular risk factors such as blood pressure, cholesterol, diabetes, and smoking
- monitoring for symptoms or signs that could suggest disease progression, such as increasing fatigue, worsening anemia, or an enlarging spleen
A small percentage of people may develop myelofibrosis or, rarely, acute leukemia after many years, but these changes are uncommon. Regular follow-up helps detect any changes early and allows your team to adapt your treatment.
With consistent care and good communication, many people with ET remain stable and active for decades.
Making sense of it
Think of your bloodstream like a construction site.
Platelets are the workers that rush in to repair any damage in the blood vessels.
In ET, too many workers show up, crowding the site and increasing the chance of mistakes or over-building.
Treatment helps reduce the crowd and keep the repair work organized and safe.
Essential thrombocythemia means your bone marrow is making more platelets than your body needs. Too many platelets can increase the chance of blood clots, and when counts are extremely high they can also lead to bleeding because the platelets do not work normally. Treatments like aspirin and medicines that lower platelet production help keep your platelet count in a safer range, reduce clot and bleeding risk, and support a long, active life.
Key takeaways
- ET is a chronic blood cancer, in which the marrow makes too many platelets
- most cases are driven by acquired gene changes, usually JAK2, CALR, or MPL mutations, and a smaller group have triple-negative ET
- the main concern is blood clots, especially in the brain, heart, lungs, legs, or abdominal veins
- very high platelet counts (often above about 1,500,000) can also cause bleeding, because platelets stop working normally and clotting proteins are used up
- risk level depends on age, clot history, and mutation status, and guides how strongly doctors recommend platelet-lowering medicines
- aspirin and cytoreductive medicines lower risk, and treatment is adjusted over time based on platelet counts and symptoms
- lifestyle changes matter, including not smoking, staying active and hydrated, and managing blood pressure, cholesterol, and diabetes
- pregnancy in et needs special planning, with changes to medications and close monitoring by a hematologist and high-risk obstetrician
- a small percentage of people progress to myelofibrosis or leukemia, which is why lifelong follow-up is important, but most people remain stable for many years
- most people with et can live long, active lives, especially when they understand the condition, follow treatment, and seek help promptly for warning symptoms
For clinicians: Read our detailed guide on how to communicate about ET to patients.