Below are three studies that collectively highlight that individuals with thalassemia trait, particularly beta-thalassemia trait, often have normal or elevated serum ferritin levels, even in the absence of transfusions or iron supplementation. This elevation is attributed to increased intestinal iron absorption, a compensatory response to ineffective erythropoiesis. One study found that up to 44% of men and 21% of women with beta-thalassemia trait had elevated ferritin, with only a minority showing true iron deficiency. Another study confirmed that while ferritin can be elevated in these individuals, transferrin saturation rarely exceeds thresholds consistent with iron overload, and co-inheritance of mild HFE mutations (e.g., H63D) did not significantly impact iron status. These findings underscore the importance of not routinely prescribing iron supplementation in patients with thalassemia trait unless iron deficiency is clearly documented. Overprescribing iron in this population risks unnecessary iron accumulation, which may lead to long-term complications. Careful evaluation of iron indices, particularly serum ferritin and transferrin saturation, is essential before initiating iron therapy.
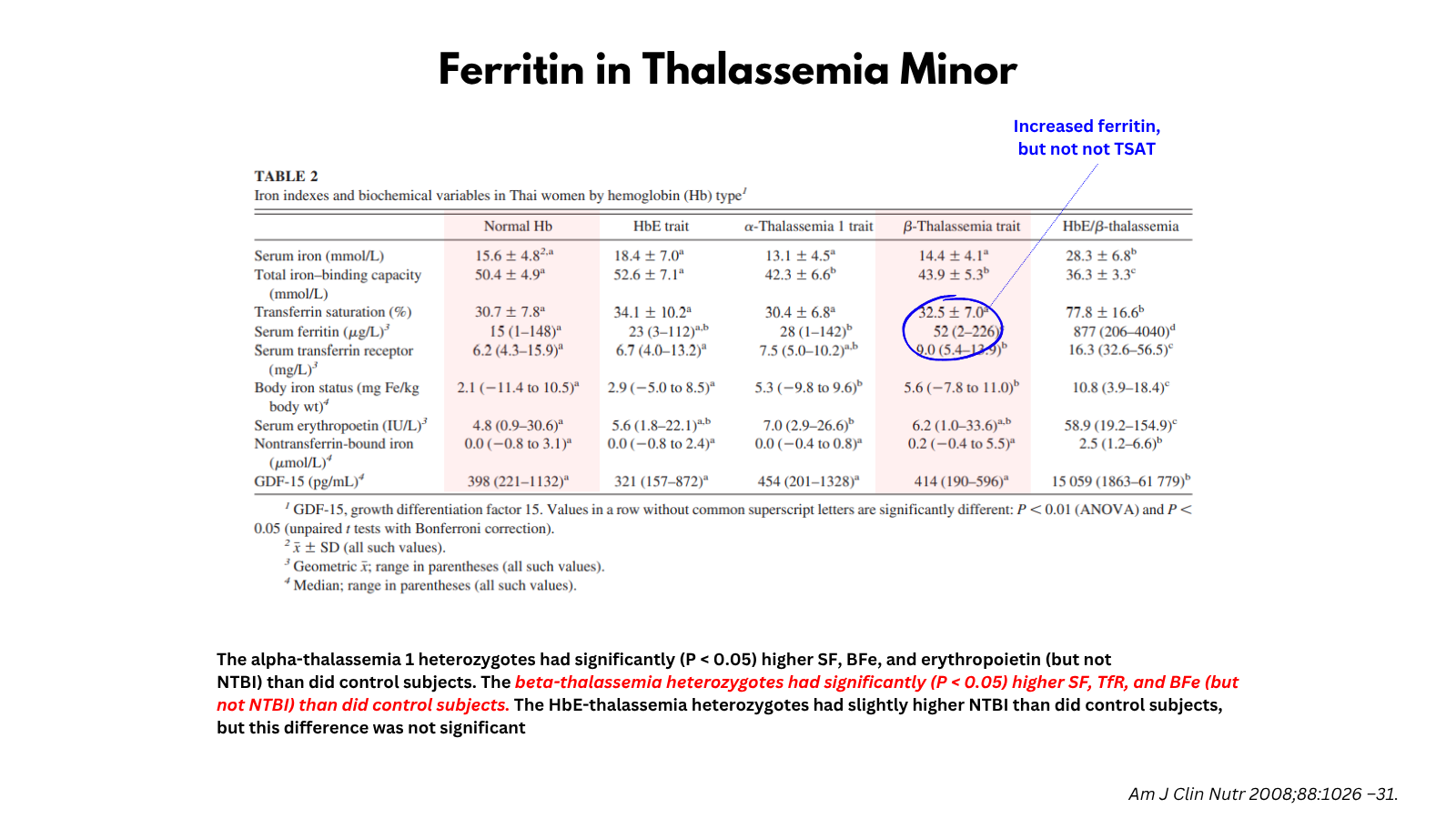
Study 1: Zimmermann et al, Iron metabolism in heterozygotes for hemoglobin E (HbE), alpha-thalassemia 1, or beta-thalassemia and in compound heterozygotes for HbE/beta-thalassemia. Am J Clin Nutr. 2008 Oct;88(4):1026-31.
Summary of key findings:
- Ferritin Levels in Thalassemia Trait (Minor):
- β-thalassemia trait: Ferritin and body iron stores were modestly elevated compared to controls.
- α-thalassemia-1 trait: Similar modest increases in ferritin and body iron stores.
- HbE trait: Ferritin levels were not significantly different from controls.
- Iron Absorption and Utilization:
- In β- and α-thalassemia traits, iron absorption was increased despite higher iron stores, indicating inappropriate regulation of iron absorption.
- Iron utilization (incorporation into erythrocytes) was ~15% lower than in controls, suggesting ineffective erythropoiesis.
- This mismatch may explain the modest increase in storage iron (i.e., ferritin) despite no clinical iron overload.
- Clinical Implications:
- Ferritin in thalassemia minor is typically normal or mildly elevated.
- In alpha-thalassemia 1 and beta-thalassemia heterozygotes with ineffective erythropoesis, dietary iron absorption is not adequately down-regulated, despite a modest increase in body iron stores.
- Routine iron supplementation or fortification should be approached cautiously in populations with high thalassemia trait prevalence.
- In thalassemia minor, elevated ferritin may not indicate iron overload but reflects mildly increased iron absorption due to ineffective erythropoiesis.

For larger image, click here.
{kind=link}
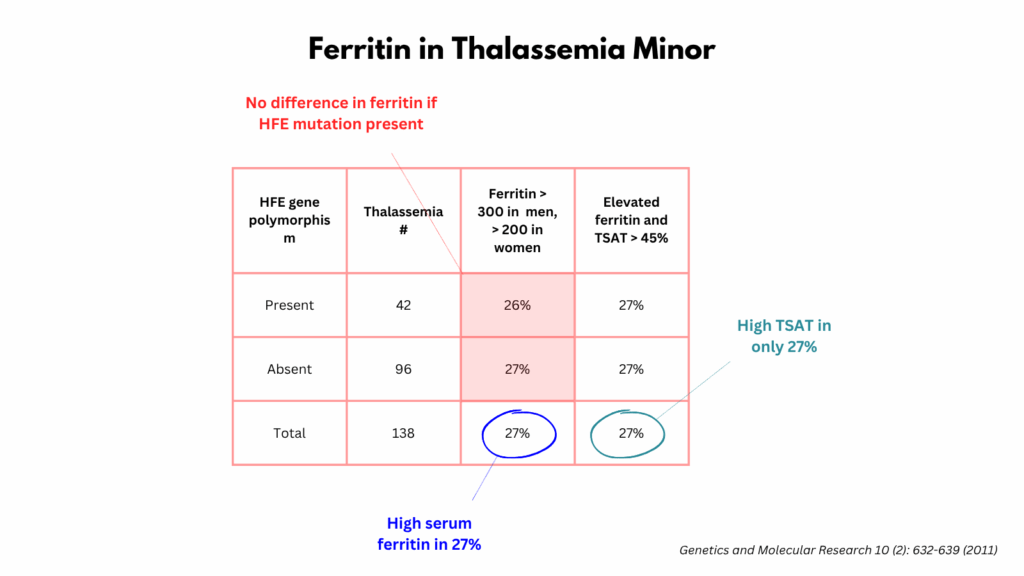
Study 2: Estevao et al. Serum ferritin and transferrin saturation levels in β⁰ and β(+) thalassemia patients. Genet Mol Res. 2011 Apr 12;10(2):632-9.
Summary of key findings:
- This study assessed serum ferritin and transferrin saturation (TSAT) levels in individuals with β⁰ and β⁺ thalassemia trait, including analysis of co-inherited HFE gene mutations (e.g., H63D, C282Y).
- Ferritin levels were variable in individuals with β-thalassemia trait, regardless of whether they had β⁰ or β⁺ mutations.
- About 27% of beta-thalassemia carriers had elevated ferritin levels, but only 7% had both elevated ferritin and TSAT >45%, a marker of iron overload.
- HFE gene mutations were found in ~30% of subjects (mostly H63D heterozygotes), but did not significantly affect ferritin or TSAT levels.
- Ferritin was higher in men and in individuals >40 years old across all groups.
- No significant difference in ferritin or TSAT between β⁰ and β⁺ traits, or between those with and without HFE mutations.
- Clinical Implications:
- Ferritin is often elevated in β-thalassemia trait, but does not necessarily indicate iron overload.
- Elevated TSAT is infrequent, even among those with high ferritin.
- Co-inherited HFE mutations (especially H63D) do not significantly worsen iron status in most β-thalassemia carriers.
- Age and sex influence ferritin more than genotype or HFE status.
For larger image, click here.
{kind=link}
Study 3: Fargion S et al, The iron status of Italian subjects with beta-thalassemia trait. Acta Haematol. 1982;68(2):109-14.
Summary of key findings:
- This study examined iron status in 140 Italian adults with beta-thalassemia trait to assess the risk of iron overload in the absence of transfusions or iron therapy.
- Key Findings:
- Serum ferritin was elevated in:
- 44% of men
- 21% of women
- Ferritin levels were significantly higher in β-thalassemia trait subjects than in healthy controls (mean 321 ng/mL in men vs. 93 ng/mL in controls; p < 0.01).
- 10% of women had low ferritin, indicating that iron deficiency can still occur, especially in menstruating females.
- A strong correlation was found between serum ferritin and desferrioxamine-induced urinary iron excretion, confirming ferritin as a reliable marker of iron stores.
- No correlation was observed between ferritin and red cell indices (MCV, Hb, MCH), suggesting that iron overload is independent of anemia severity.
- Serum ferritin was elevated in:
- Conclusions:
- Individuals with beta-thalassemia trait, especially men, may develop iron overload due to increased intestinal iron absorption, even without transfusion or iron therapy.
- Serum ferritin is the most sensitive indicator of iron overload in this population.
- Routine iron supplementation in beta-thalassemia trait should be avoided unless iron deficiency is confirmed.

For larger image, click here.
{kind=link}