Differential diagnosis of polycythemia/erythrocytosis. First branch point separates polycythemia/erythrocytosis into relative and absolute. Relative polycythemia/erythrocytosis indicates a reduction in plasma volume, whereas absolute polycythemia/erythrocytosis arises from an elevated red blood cell mass. Relative polycythemia/erythrocytosis may be transient from vomiting, diarrhea or diuretics, or chronic (Gaisbock’s syndrome). Absolute polycythemia/erythrocytosis is then classified according to whether it is primary or secondary. In primary absolute polycythemia/erythrocytosis, there is autonomous growth of red blood cell progenitors either from congenital mutations in erythropoietin receptor gene or in the setting of acquired polycythemia vera. In secondary absolute polycythemia/erythrocytosis, the driver for increased red cell production lies outside the erythroid precursor cell, typically in the form of elevated erythropoietin levels. In some cases, erythropoietin levels are “appropriately” elevated owing to reduced oxygen delivery to the peritubular cells of the kidney that produce the hormone. In other cases, erythropoietin levels are “inappropriately” elevated independent of oxygen delivery to erythropoietin-producing cells of the kidney.
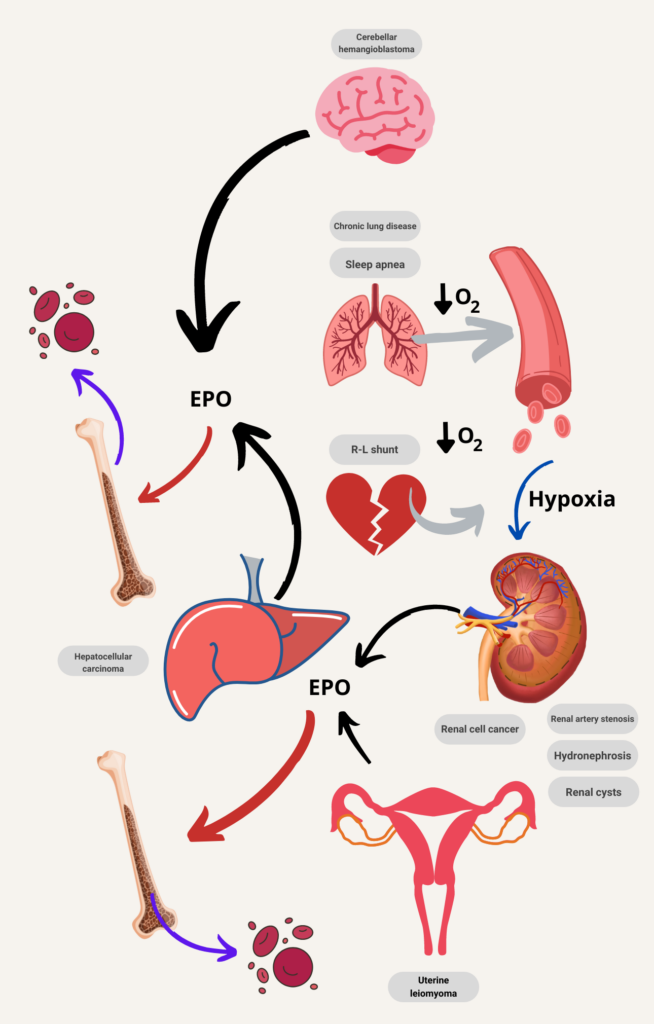
Diagnostic flow chart from organ perspective. EPO, erythropoietin.